A7 · Clinical conditions
Peri-implantitis: early signs, prevention, and treatment
Peri-implantitis is the leading cause of late implant failure, and most of it is preventable. This article sets out the diagnostic criteria — bleeding on probing, pockets at or above 6mm, bone loss over 3mm — explains why peri-implant mucositis is the reversible warning to act on, names the real risk modifiers including smoking and uncontrolled diabetes, and walks the staged treatment ladder from non-surgical debridement to explantation.
- Published
- 2026-05-20
- Reading time
- 9 minutes
- Author
- Prof. Robert Ćelić
- Section
- Clinical conditions
At our specialist clinic for dental implants in Zagreb, working with Swedish patients on long-term implant outcomes, the condition we spend the most prevention time on is peri-implantitis — the leading cause of late implant failure. The honest version: it is more common than many clinics admit, the early-stage form is fully reversible, and it is almost always preceded by warning signs a patient can see. The patients who know what to watch for keep their implants for decades.
What is peri-implantitis?
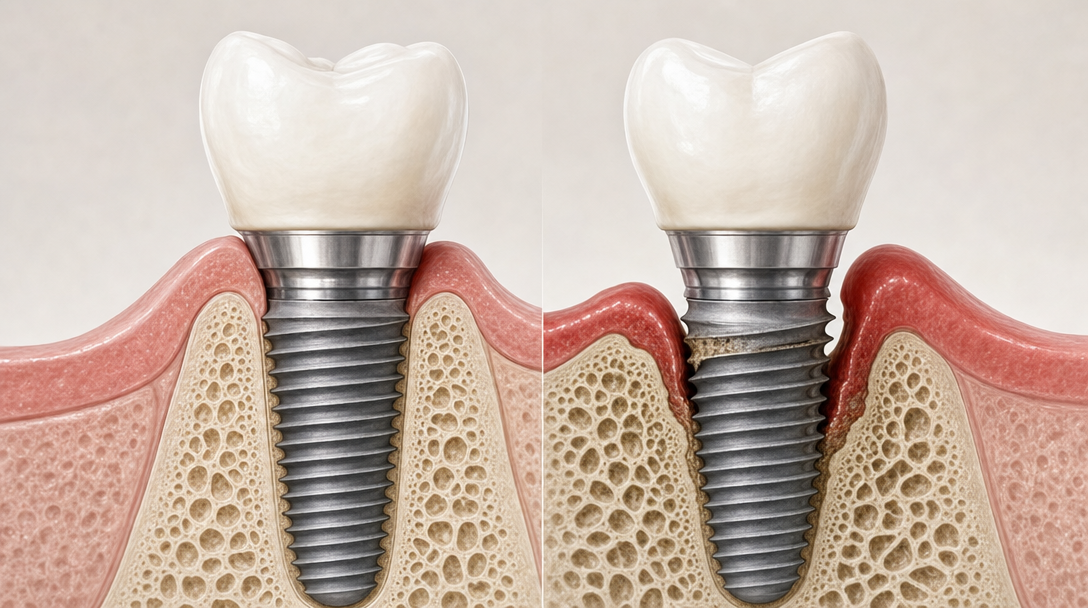
Peri-implantitis is an inflammatory condition affecting the soft and hard tissues around a dental implant, characterised by progressive loss of supporting bone. Per the 2018 World Workshop consensus — the current peer-reviewed gold standard for peri-implant disease classification — the diagnosis requires three findings together:
- · Bleeding on probing (BoP) and/or suppuration (pus) on gentle probing
- · Increased probing depth compared to baseline measurements
- · Radiographic bone loss beyond the initial bone remodelling expected after implant placement
When baseline radiographs are not available, modern case-definition criteria (Renvert 2018) use a numeric threshold combining three findings:
- · Bone level at least 3 mm apical to the most coronal intraosseous part of the implant
- · BoP or suppuration on gentle probing
- · Probing depth at least 6 mm
The distinction that matters clinically. Peri-implantitis has a reversible precursor: peri-implant mucositis — inflammation in the soft tissue without bone loss. The distinction is load-bearing:
- · Mucositis is reversible with improved hygiene and professional cleaning
- · Peri-implantitis requires surgical intervention in most cases and may eventually require implant removal
A note on Swedish terminology: Socialstyrelsen and SBU lock the single-word form periimplantit (no hyphen) as canonical clinical Swedish. We use it that way throughout this article.
Early signs — and why peri-implant mucositis is the warning before the failure
This is the most important section for patients. The transition from healthy to mucositis to peri-implantitis is not always linear — peri-implantitis often progresses in bursts, faster and more episodically than periodontitis around natural teeth. The patient who catches the warning at the mucositis stage protects the implant. The patient who waits until it hurts often loses it.
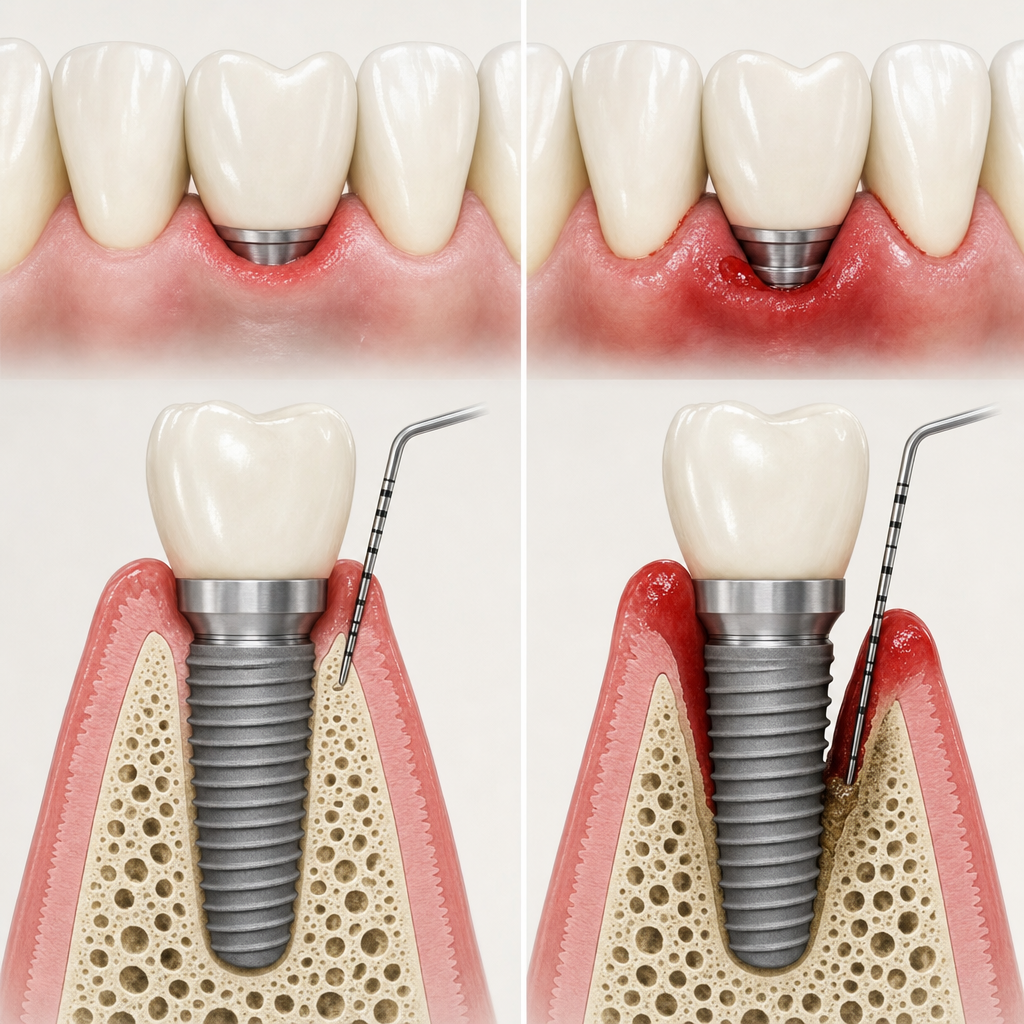
What peri-implant mucositis looks like — the early warning:
- · Gingival redness around the implant, compared to the healthy pink tissue elsewhere in your mouth
- · Bleeding when brushing or flossing near the implant — even mild bleeding is a sign
- · Slight tenderness or sensitivity around the implant gum line
- · Bad taste or mild halitosis localised to the implant
- · No pain at this stage — and that is exactly why it gets missed
What early peri-implantitis looks like — when mucositis has progressed:
- · All of the above, plus:
- · Visible gingival recession — the implant "looks longer" than before
- · Deeper pocket detectable on probing (clinical-exam finding, not a self-check)
- · Bone loss visible on bitewing X-ray (clinical finding)
Late peri-implantitis — pus discharge, pain on chewing, eventually implant mobility (rarely until very late, because implants do not loosen the way natural teeth do until bone loss is substantial).
A clinically useful nuance about bleeding. Absence of bleeding on probing at an implant has a high negative predictive value for future bone loss — implants without BoP rarely show disease progression (Monje et al. 2021). Presence of BoP alone is less specific; it must be interpreted together with probing depth and radiographs. An isolated bleeding episode is not a panic signal. Persistent bleeding plus deeper pockets is.
What we ask Swedish patients to do. Monthly self-check at home: pink, intact, non-bleeding gingiva around the implant when brushing means healthy. Anything else means book a check-up — in person at the clinic if you happen to be in the area, or with your own dentist in Sweden if not (we provide the treatment record on request).
For the biology this is the failure mode of, see our how osseointegration actually works article.
What causes it — the modifiable and the unmodifiable factors
The honest picture: most risk is behaviour, not biology. Three categories — strongly modifiable, moderately modifiable, and clinic-controlled — let you see what you actually control. Modern epidemiology comes from the Derks & Tomasi 2015 systematic review, reporting weighted-mean prevalence around 22% at the patient level across modern studies.
Strongly modifiable (you control these directly).
- · Smoking is the single biggest modifiable risk — it roughly doubles to triples the peri-implantitis risk compared to non-smokers. Cessation reduces risk significantly within months and normalises within years.
- · Oral hygiene — daily brushing plus interdental cleaning with implant-specific floss or brushes cuts risk dramatically.
- · Regular maintenance and recall — the modern recommendation is 3–6 monthly professional maintenance, not annual. Regular maintenance substantially improves long-term implant survival compared to irregular attendance. The "burst" progression pattern is the reason short recall intervals matter so much.
- · Diabetes control — well-controlled diabetes is not an exclusion; poorly controlled diabetes meaningfully elevates risk.
Moderately modifiable.
- · History of periodontitis on natural teeth is one of the strongest predictors. Meta-analyses (Sgolastra et al. 2015; Chrcanovic et al. 2014) show a clearly elevated peri-implantitis risk — on the order of twofold or more — in patients with a history of treated periodontitis. Treated periodontitis is not a contraindication, but it does change the prevention protocol — shorter recall intervals, stricter hygiene.
- · Bruxism / tooth grinding — mechanical overload contributes; we recommend night guards.
- · Diet — high-sugar diet promotes plaque accumulation around implants the same way it does around natural teeth.
Less modifiable — clinic-controlled.
- · Implant surface modification. Extremely rough or porous legacy surfaces (some early plasma-sprayed and hydroxyapatite-coated designs) were associated with higher peri-implantitis once exposed. The modern moderately rough surfaces we use (SLA, SLActive — Sa around 1–2 µm) are mainstream; their peri-implantitis risk is driven more by patient and prosthetic factors than by the surface itself.
- · Cement-retained versus screw-retained prosthetics. Excess cement is a well-established trigger (Linkevicius et al. 2013; Korsch et al. 2014). At our dental implants in Croatia clinic, we use screw-retained prosthetics where clinically possible and meticulously clean cement margins when cement is unavoidable.
- · Bone augmentation history — sites that needed augmentation have moderately higher long-term risk; manageable with attentive hygiene.
At consultation, every implant candidate gets a risk profile assessment: smoking status, periodontitis history, diabetes control, bruxism habits. Patients in the higher-risk group get an individualised prevention protocol — more frequent professional cleaning, prescription chlorhexidine rinse phases, a custom night guard if indicated.
Honest framing:
Some risk is biology. Most risk is behaviour. The implant that fails to peri-implantitis eight years after placement is usually an implant whose owner stopped doing the things that protect it.
How we prevent it — and what treatment looks like if it occurs
Prevention protocol (what we do for every Swedish patient):
- · Risk profile assessment at consultation (smoking, periodontitis history, diabetes, bruxism)
- · Pre-implant periodontal treatment if natural teeth show active disease — peri-implantitis risk is markedly higher with active periodontitis
- · Implant surface selection appropriate to the risk profile (SLA / SLActive standard)
- · Screw-retained prosthetics where clinically possible to avoid cement-margin risk
- · Written home-care protocol — implant-specific interdental brushes, hygiene technique demonstration, a chlorhexidine rinse phase for the first four weeks
- · 3–6 monthly professional cleaning and radiographic monitoring — at Ars Salutaris when travel is convenient, or with the patient's own dentist in Sweden when not (we provide the necessary records on request)
Treatment if peri-implantitis occurs — staged by severity (per Berglundh et al. 2018 framework and the EFP S3 guideline, Herrera et al. 2023):
Stage 1 — Peri-implant mucositis (no bone loss).
- · Professional cleaning around the implant
- · Improved home care
- · Chlorhexidine rinse phase (2–4 weeks)
- · Re-evaluation at 4–6 weeks
- · Fully reversible in most cases
Stage 2 — Early peri-implantitis (bone loss under 2 mm beyond baseline).
- · Non-surgical: subgingival cleaning with mechanical and air-abrasive devices, local antimicrobials, sometimes systemic antibiotics
- · Re-evaluation at 8–12 weeks
- · Honest framing per EFP S3 guideline. Non-surgical therapy at this stage is initial treatment, not generally curative for established peri-implantitis. It controls inflammation and is the right starting point. Established bone loss often requires surgical management.
Stage 3 — Moderate peri-implantitis (bone loss 2–4 mm).
- · Surgical access flap procedure
- · Implant surface decontamination (titanium curettes, glycine air-polishing)
- · Bone regenerative procedure if defect geometry permits — contained intrabony defects typically yield 2–4 mm mean probing-depth reduction and clinical attachment gain; complete defect fill is less predictable
- · Adjunctive enamel matrix derivative (EMD) in regenerative surgery — regenerative treatment can reduce pocket depth and recover some bone in selected contained defects (Ramanauskaite et al. 2023)
- · 4–6 month healing before re-evaluation
Stage 4 — Advanced peri-implantitis (bone loss over 4 mm, mobility, or abscess).
- · Mobility implies loss of osseointegration — implant removal is indicated
- · Re-augmentation is possible after healing
- · New implant placement after 3–6 months
- · The choice between resective surgery and explantation depends on defect pattern, implant position, and prosthetic demands — not on a hard millimetre threshold alone
Adjunctive therapies with limited but real evidence. Photodynamic therapy and dental lasers offer short-term improvements in BoP and pocket depth but no consistent long-term advantage over conventional therapy. The EFP S3 guideline does not recommend them as standalone treatments for peri-implantitis. Peri-implant crevicular fluid biomarkers (IL-1β, MMP-8) and microbiome profiling are promising research tools, but they are not yet part of standard chairside diagnostic criteria.
Honest framing per voice guide §5:
We do not pretend peri-implantitis is rare. Modern longitudinal cohorts show roughly one in five patients develop peri-implantitis over a 5–10 year period. The reversible precursor — mucositis — is even more common. The older "1–7%" figures from the early 2000s reflected looser definitions and shorter follow-up; the modern numbers are higher because the definitions are sharper, not because implants got worse. What we can promise is the prevention protocol that reduces individual risk and the early detection that keeps reversible cases reversible.
Peri-implantitis is the condition implant patients should worry about strategically — and only strategically. Worry enough to maintain hygiene, attend 3–6 monthly check-ups, stop smoking if you smoke. Do not worry enough to be afraid of implants — the modern long-term success rates are excellent for patients who follow the prevention protocol. If you have implants from a previous treatment and want a peri-implant health assessment from a named specialist with a verifiable EDA-Expert credential, Prof. Robert Ćelić, European Expert in Implantology reviews remote-patient cases via CBCT and video consultation. No deposit, no commitment.
References
Sources referenced.
- Berglundh T, Armitage G, Araujo MG, et al. (2018) — Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop. J Periodontol 2018;89(Suppl 1):S313–S318. PMID 29926955. External link in the text.
- Renvert S, Persson GR, Pirih FQ, Camargo PM (2018) — Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J Clin Periodontol 2018;45(Suppl 20):S278–S285. PMID 29926953. Cited in the text.
- Derks J, Tomasi C (2015) — Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol 2015;42(Suppl 16):S158–S171. PMID 25495683. External link in the text. Weighted mean prevalence ~22% at patient level.
- Monje A, Amerio E, Farina R, et al. (2021) — Significance of probing for monitoring peri-implant diseases. Int J Oral Implantol (Berl) 2021;14(4):385–399. PMID 34726848. Cited in the text (BoP as a clinical indicator).
- Sgolastra F, Petrucci A, Severino M, et al. (2015) — Periodontitis, implant loss and peri-implantitis. A meta-analysis. Clin Oral Implants Res 2015;26(4):e8–e16. PMID 24382358. Cited in the text.
- Chrcanovic BR, Albrektsson T, Wennerberg A (2014) — Periodontally compromised vs. periodontally healthy patients and dental implants: a systematic review and meta-analysis. J Dent 2014;42(12):1509–1527. PMID 25283479. Cited in the text.
- Linkevicius T, Puisys A, Vindasiute E, et al. (2013) — Does residual cement around implant-supported restorations cause peri-implant disease? A retrospective case analysis. Clin Oral Implants Res 2013;24(11):1179–1184. PMID 22882700. Cited in the text.
- Korsch M, Obst U, Walther W (2014) — Cement-associated peri-implantitis: a retrospective clinical observational study of fixed implant-supported restorations. Clin Oral Implants Res 2014;25(7):797–802. PMID 23600620. Cited in the text.
- Herrera D, Berglundh T, Schwarz F, et al. (2023) — Prevention and treatment of peri-implant diseases — The EFP S3 level clinical practice guideline. J Clin Periodontol 2023;50(Suppl 26):4–76. PMID 37271498. Cited in the text.
- Ramanauskaite A, Cafferata EA, Begic A, Schwarz F (2023) — Surgical interventions for the treatment of peri-implantitis. Clin Implant Dent Relat Res 2023;25(4):682–695. PMID 36419243. Cited in the text (regenerative/reconstructive surgery).
Read next
Three pages worth your time.
The Pezo–Ćelić Protocol
Dental implants in Croatia — 20-year written guarantee
The full offer stack, dual guarantees, and surgeon-team accountability detailed.
Named credentials
Prof. Ćelić, European Expert in Implantology
Full Professor at University of Zagreb. BDIZ EDI certified. 916+ citations.
Related article
Osseointegration — how an implant fuses with the jawbone
How a healthy implant is supposed to bond with bone, so the warning signs of peri-implantitis read clearly against it.
Frequently asked questions
What is peri-implantitis?
What is the difference between peri-implant mucositis and peri-implantitis?
What are the early warning signs of peri-implantitis?
How common is peri-implantitis?
How can I prevent peri-implantitis?
Can peri-implantitis be treated, or do I lose the implant?
Ready when you are
Want a CBCT-based assessment from a named specialist?
A free 30-minute consultation. Send us your X-rays or current treatment plan. We will review it, give you our honest assessment, and confirm whether you are a candidate. If we do not think we are the right fit for your case, we will say so.
No deposit. No commitment.