A7 · Clinical conditions
Osseointegration: how a dental implant fuses with the jawbone
Osseointegration is the biological lock that turns a titanium screw into a load-bearing part of your jaw. This article walks through the Brånemark definition, the three integration phases from mechanical fixation to osteoblast-driven biology, what patient, clinic, and material factors decide the outcome, and how stability-guided loading per the 2022 EAO consensus shapes when an implant is safe to restore.
- Published
- 2026-05-20
- Reading time
- 9 minutes
- Author
- Prof. Robert Ćelić
- Section
- Clinical conditions

At our specialist clinic for dental implants in Zagreb, working with Swedish patients flying in for treatment, the question we hear most often early in consultation is some version of: how exactly does an implant fuse with the bone? The answer is osseointegration — a biological process that turns a titanium screw into a structural part of your jaw. This article explains how it works, what affects the outcome, and what happens when it does not.
What is osseointegration?
Osseointegration is the direct structural and functional connection between living bone and the surface of a load-bearing implant. The definition was first formulated by Swedish researcher Per-Ingvar Brånemark in the late 1960s (Brånemark et al., 1969). In simpler terms: the jawbone grows directly against the titanium surface, with no soft tissue in between. That direct contact is what allows an implant to function like a real tooth root — to carry chewing forces decades after placement.
This is the line between a successful implant (osseointegrated, stable for decades) and a failed one (encapsulated in fibrous tissue, loose within months). A correctly osseointegrated implant becomes biomechanically indistinguishable from a natural tooth root under load. A failed one moves, hurts, and eventually has to come out.
Osseointegration is not an event that happens during surgery. It is a biological process that unfolds over weeks after the implant is placed. Understanding the timeline, and the factors that affect it, is the difference between informed consent and uninformed surprise.
How the biological process works
Osseointegration unfolds in three overlapping phases. Modern surface-modified titanium implants reach stable integration in roughly 4–6 weeks in the lower jaw and 6–8 weeks in the upper jaw under good conditions. The historical 8–16 week timeframe from Brånemark's original work still applies to compromised cases — low-density bone, complex grafts, or smokers. It is no longer the default for healthy candidates.
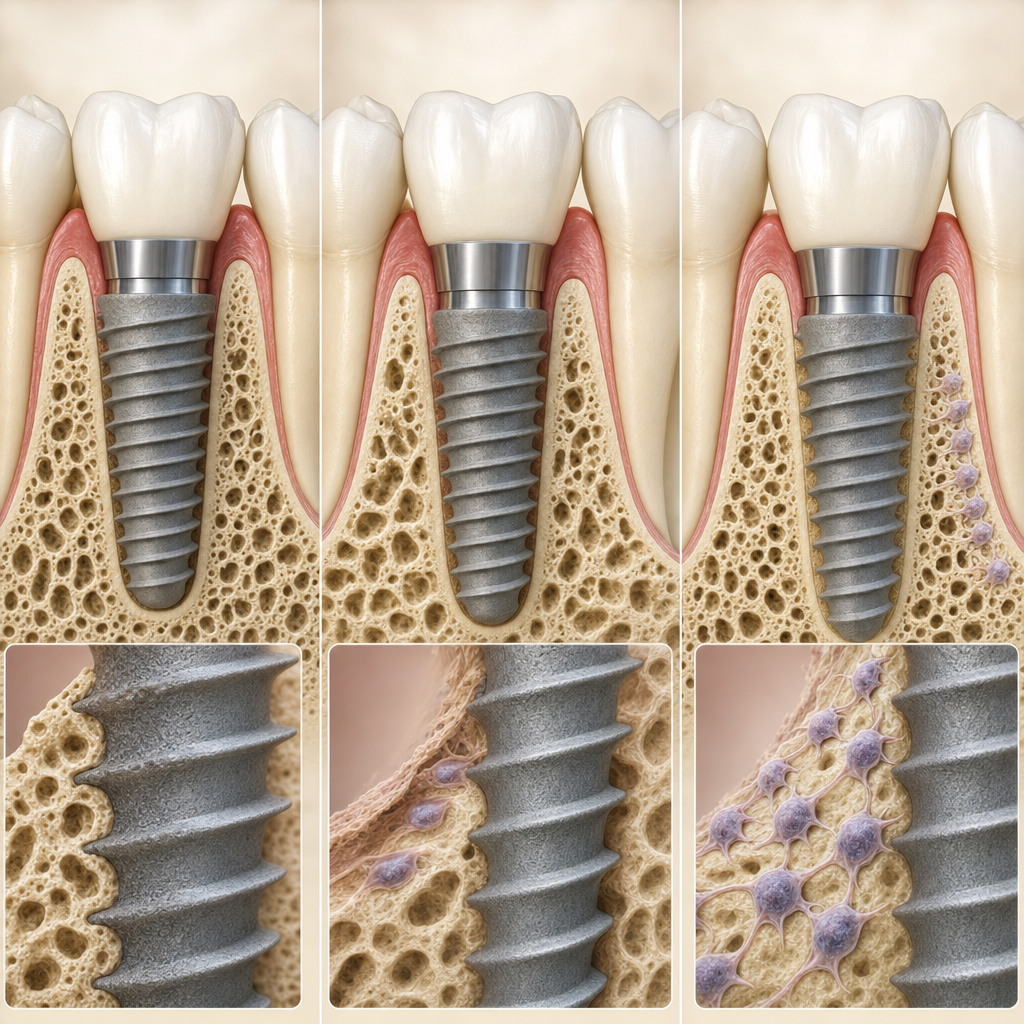
Phase 1 — mechanical fixation. The implant is screwed into a precisely prepared site in the bone. The threads compress against the surrounding bone, creating immediate primary stability. This is friction-fit — purely mechanical, held the way a screw is held in dense wood. The implant cannot carry real chewing load at this stage, but it is stable enough for the next phase to begin.
Phase 2 — early bone remodelling (week 1 to 3). The bone around the implant begins to remodel in response to the surgical insertion. Mechanical stability temporarily decreases as the bone resorbs slightly before regenerating. This "stability dip" usually bottoms around week 2 or 3 and is part of the normal pattern, not a complication. Patients sometimes notice an implant that felt rock-solid at placement become slightly mobile around this time. That is the dip; it resolves on its own.
Phase 3 — biological integration (week 4 onwards). Osteoblasts — the body's bone-building cells — deposit new bone directly onto the implant surface. The body recognises titanium's passive oxide layer (TiO₂, only 2–10 nanometres thick, self-repairing within milliseconds) as inert. Bone grows toward it rather than walling it off. Hydroxyl groups on that oxide layer attract calcium ions from the blood, nucleating biological apatite — natural bone mineral — directly on the titanium. There is no glue and no fibrous tissue between bone and implant (Albrektsson et al., 1981).
Modern hydrophilic surfaces (SLActive, Roxolid, and similar treatments) can shorten this early healing phase compared with older smooth-machined titanium. In practice, early healing tends to be faster, particularly in the upper jaw.
The current European Association for Osseointegration (EAO) consensus from 2022 moved away from fixed-calendar healing protocols toward stability-guided loading. Implants that reach adequate stability values may be loaded earlier; those that have not may need extended healing. Calendar-based loading is now the older standard, not the contemporary one.
What factors affect the outcome?
Three categories of factors shape whether an implant osseointegrates successfully. Some are about you, some are about the clinic, and some are about the implant itself.
Patient factors. Bone density is the most-discussed of these. The Lekholm-Zarb classification (types I to IV) describes how dense your jawbone is — type I is dense cortical, type IV is soft and primarily trabecular. Type IV bone reduces survival, but modern hydrophilic surfaces have narrowed this gap markedly. Soft bone was historically more challenging to treat, but with contemporary SLActive-type surfaces the gap has narrowed considerably. Soft bone is no longer the contraindication it once was.
General health matters next. With well-controlled diabetes, implant survival is broadly comparable to non-diabetics. Poorly controlled diabetes can affect the outcome negatively and raises the risk, so blood sugar should be stable before treatment. Well-controlled diabetes is not an exclusion. Bisphosphonate use is similarly nuanced. Oral bisphosphonate under three years is essentially safe; intravenous therapy beyond two years carries materially elevated risk and warrants caution.
Smoking is a genuine, well-documented risk factor. Smoking roughly doubles to triples the risk of peri-implantitis and impairs healing, with heavy smokers at the highest risk. Cessation does work — risk falls gradually after quitting, and heavy smokers have the most to gain from stopping. We cover the smoking-implant relationship in deeper detail in a separate post.
Bruxism, or tooth grinding, is often described as a contraindication, but the modern evidence is more specific. Early failure rates in bruxers are comparable to non-bruxers. The problem is long-term mechanical complications, which are more common in patients who grind. Bruxism is not an early-failure risk; it is a long-term mechanical risk. We manage it with splinted prostheses, restricted cantilever length, and a mandatory night guard. For broader patient-side context on what life with implants looks like, 1177.se patient information on artificial teeth is the Swedish institutional reference.
Clinic factors. Surgical technique matters concretely. Drilling generates heat; bone exposed to temperatures above 47°C for more than a minute undergoes irreversible thermal necrosis (Eriksson & Albrektsson, 1983). Adequate irrigation and disciplined bur speed prevent this. Primary stability at placement is measured with an ISQ value. Higher ISQ values are associated with better conditions for early loading, and the threshold is typically somewhat lower in the upper jaw because maxillary bone is generally less dense.
Material factors. Implant brand and prosthetic fit precision both shape outcomes. Modern research puts 10-year survival for dental implants high — a systematic review and meta-analysis (Howe et al. 2019) reports around 93 to 96% implant survival at ten years, with some variation depending on where in the jaw the implant sits. All EU CE-marked systems we use — Straumann, Nobel Biocare, ICX — fall within this range. The final piece is the crown. At our dental implants in Croatia clinic, Naturaldent's in-house CAD/CAM lab maintains a tight fit tolerance on the prosthetic side. This reduces micro-movement under load and protects the integration over decades of use.
When osseointegration fails
Most implants succeed. A minority do not. Failure modes split cleanly into early and late.
Early failure — the first weeks to months after placement — is uncommon in modern practice — on the order of a few percent of cases, lower than the rates cited in older textbooks. The improvement reflects better surface technology, CBCT-based three-dimensional planning, and disciplined surgical protocols. Early failure typically results from one of three causes. Infection at the surgical site. Micro-movement during the healing phase, often from a provisional crown placed too early. Or inadequate primary stability at placement — soft bone, suboptimal surgical technique. When an early failure happens, the implant is removed. The site heals for three to six months, and a new implant is usually possible — sometimes preceded by bone augmentation.
Late failure — months to years after the implant has integrated and been loaded — is the more common pattern in long-term data. The dominant late-failure mechanism is peri-implantitis, an inflammatory condition affecting the soft tissue and bone around a previously stable implant. Peri-implantitis affects roughly a fifth of patients — about 22% (Derks & Tomasi 2015) — over a five- to ten-year period. That is significant but not catastrophic; the majority are caught at early stages through routine recall and treated successfully. The post-integration phase is where peri-implantitis emerges, and we cover what to expect during that period in our healing time week by week explainer. Other late mechanisms account for the rest: mechanical overload from untreated bruxism, prosthetic complications such as a loose abutment screw or a fractured crown.
Honest framing matters here. Early failure is uncommon, on the order of a few percent of cases in modern data. Long-term, peri-implantitis affects a meaningful minority of patients. It is largely modifiable through hygiene, recall compliance, and risk-factor management. No clinic can guarantee 100% survival. What we can do is minimise the modifiable risk factors and design the prosthetic side to protect the biology underneath. When failure does happen, recovery — explantation, healing, often re-implantation — is a well-established protocol, not a catastrophe.
Osseointegration is largely about biology, but also about a number of measurable clinical decisions — surgeon training, CBCT-based planning, disciplined surgical technique, prosthetic fit precision. Those decisions are often the difference between an implant that lasts five years and one that lasts twenty-five. If you are considering implant treatment, a second opinion from a named specialist can help. We offer a free 30-minute consultation to verify your candidacy. Prof. Robert Ćelić, European Expert in Implantology reviews cases personally. No deposit, no commitment.
References
Sources referenced.
- Brånemark P-I et al. (1969) — Intra-osseous anchorage of dental prostheses. I. Experimental studies. Scand J Plast Reconstr Surg 1969;3(2):81–100. External link in H2.1.
- Albrektsson T, Brånemark P-I, Hansson H-A, Lindström J (1981) — Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop Scand 1981;52(2):155–170. External link in H2.2.
- 1177.se — Konstgjorda tänder. Sweden's national health information service, patient-facing lay reference. External link in H2.3.
- Howe MS, Keys W, Richards D (2019) — Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J Dent 2019;84:9–21. PMID 30904559. Cited in the text (material factors).
- Derks J, Tomasi C (2015) — Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol 2015;42(Suppl 16):S158–S171. PMID 25495683. Cited in the text.
- Eriksson AR, Albrektsson T (1983) — Temperature threshold levels for heat-induced bone tissue injury. J Prosthet Dent 1983;50(1):101–107. In-text only.
- Lekholm U, Zarb GA (1985) — Patient selection and preparation. In: Brånemark P-I, Zarb GA, Albrektsson T, eds. Tissue-Integrated Prostheses. Quintessence Publishing, 1985:199–209. In-text only.
- European Association for Osseointegration (EAO) 2022 consensus — stability-guided loading. In-text only.
Read next
Three pages worth your time.
The Pezo–Ćelić Protocol
Dental implants in Croatia — 20-year written guarantee
The full offer stack, dual guarantees, and surgeon-team accountability detailed.
Named credentials
Prof. Ćelić, European Expert in Implantology
Full Professor at University of Zagreb. BDIZ EDI certified. 916+ citations.
Related article
Bone augmentation before a dental implant
What to do when there is not enough bone for an implant to integrate into in the first place.
Frequently asked questions
What is osseointegration in simple terms?
How long does a dental implant take to fuse with the jawbone?
Can I have implants if I have diabetes?
Does bruxism (tooth grinding) mean I can't get implants?
What is the long-term survival rate for dental implants?
What happens if an implant fails?
Ready when you are
Want a CBCT-based assessment from a named specialist?
A free 30-minute consultation. Send us your X-rays or current treatment plan. We will review it, give you our honest assessment, and confirm whether you are a candidate. If we do not think we are the right fit for your case, we will say so.
No deposit. No commitment.