A7 · Clinical conditions
Sinus lift before a dental implant: when it's needed, how it works
A sinus lift adds vertical bone in the upper back jaw so an implant has structure to anchor in. This article covers the residual-height threshold that triggers the procedure, the lateral window versus transcrestal approaches, graft material choices, the real risks including Schneiderian membrane perforation and sinusitis, and when a short 6-8mm implant lets a patient skip the surgery entirely.
- Published
- 2026-05-20
- Reading time
- 8 minutes
- Author
- Prof. Robert Ćelić
- Section
- Clinical conditions

At our specialist clinic for dental implants in Zagreb, working with Swedish patients flying in for upper-jaw implant treatment, the second most common conversation we have at consultation is some version of: the X-ray shows I don't have enough bone — does that mean I can't get implants? The honest answer is almost always: you can, but you may need a sinus lift first. Here is what that actually means.
What is a sinus lift, and why do some implant patients need one?
A sinus lift — formally, sinus floor elevation — is a bone augmentation procedure performed in the posterior maxilla (the upper back jaw) to increase the available vertical bone height for an implant.
The anatomy: above the upper back teeth sits the maxillary sinus, an air-filled cavity inside the skull. The bone between the floor of that sinus and your gum line is naturally thinner here than anywhere else in the jaw. That is the bone an implant needs to anchor in. When you lose an upper back tooth, the sinus gradually expands downward into the empty space over months and years. The bone thins further. By the time you want an implant, there may not be enough vertical bone left for the implant to hold.
A sinus lift restores that height. The surgeon gently lifts the thin membrane lining the sinus floor (the Schneiderian membrane) and packs bone graft material into the space created underneath. Over months, your body integrates the graft into native bone, and the site becomes implantable.
Sinus augmentation is needed in a substantial share of posterior upper-jaw cases. Prevalence depends on patient age and how long the upper back teeth have been missing. It is among the most routine bone augmentation procedures in modern implant dentistry, with documented predictability over more than three decades of clinical use (Pjetursson et al., 2008).
When the upper jaw doesn't have enough bone height
The clinical decision is based on residual bone height (RBH) — the vertical bone available between your alveolar ridge and the sinus floor — measured on a CBCT (cone-beam CT) scan. Below are working ranges; primary stability achievable at the implant site and individual anatomy matter as much as the raw millimetres.
- · RBH ≥8–10 mm: sinus lift often unnecessary. Standard implant placement is feasible, especially with modern shorter implants.
- · RBH 5–8 mm: the implant can usually be placed in the same session as a transcrestal (Summers) sinus lift, achieving a modest 1–4 mm gain.
- · RBH 3–5 mm: the lateral window approach is appropriate, often with simultaneous implant placement if primary stability of at least 25–30 Ncm is achievable.
- · RBH below 3–4 mm: the lateral window in two stages. Graft first, implant 4–9 months later after CBCT confirms integration.
The bone loss in this region is rarely about poor hygiene. The causes are usually some combination of tooth extraction without immediate bone preservation, long-term edentulism, periodontal disease before extraction, and natural age-related sinus expansion.
The mandatory tool is CBCT. A 2D panoramic X-ray cannot show the three-dimensional anatomy needed to plan a sinus lift safely. CBCT-based planning is part of our standard consultation for any patient considering dental implants in Croatia — it is the diagnostic foundation, not an upsell.
A real modern alternative worth knowing about. Short implants (6 mm) can perform comparably to sinus augmentation with longer implants over three to five years. The condition: RBH around 6–8 mm and moderate occlusal load. Multiple RCTs and systematic reviews support this option. It is increasingly a valid plan B — not a workaround, but a different valid treatment plan. We discuss it openly with patients whose anatomy permits.
Honest framing. A sinus lift is not "extra surgery clinics push to make money." It is a clinical necessity when bone height falls below the threshold above. Skipping it when it is needed leads to implant failure within months. Performing it when it is not needed wastes time and money. The CBCT, not the brochure, decides.
How the procedure works — lateral vs transcrestal approach
There are two real techniques. Each has clear indications.
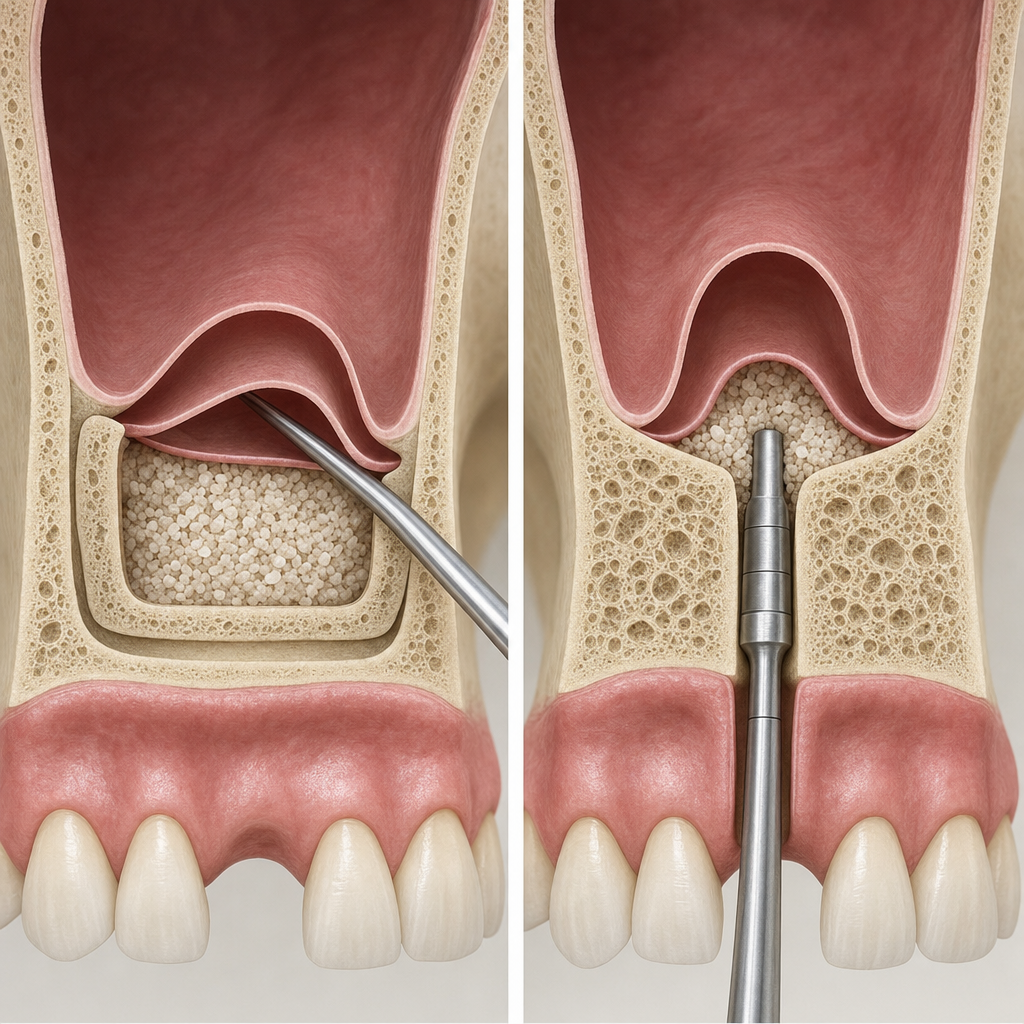
Lateral window technique (a refinement of the Caldwell-Luc approach):
- · A small bony window is cut in the lateral wall of the maxilla above the alveolar ridge
- · The Schneiderian membrane is carefully elevated from the sinus floor
- · Bone graft material is packed into the created space — autologous bone, allograft, xenograft (most commonly Bio-Oss), or a synthetic substitute
- · A collagen membrane covers the window
- · Indications: RBH below 4–5 mm, when a large vertical gain is needed, when sinus septa or complex anatomy require direct visualisation
- · Healing: 4–9 months before delayed implant placement. Simultaneous placement is possible at RBH 3–5 mm if primary stability is adequate.
- · Membrane perforation risk: ~15–20% in experienced hands (older series report rates up to around 40%). Almost always managed intraoperatively with a collagen patch; the procedure continues normally.
Transcrestal (Summers / osteotome) technique:
- · The implant osteotomy is prepared as usual but stopped 1–2 mm short of the sinus floor
- · An osteotome is used to gently fracture and push the sinus floor upward — a 1–4 mm gain reliably. Balloon-assisted and hydraulic modifications can sometimes achieve slightly more
- · Bone graft is pushed through the same access
- · The implant is placed simultaneously
- · Indications: RBH 5–8 mm, modest vertical gain needed, favourable sinus anatomy on CBCT
- · Membrane perforation risk: ~3–5% in experienced hands but technique-sensitive
Graft materials. The honest answer from the literature is that no single biomaterial consistently outperforms the others for new bone formation. Preserving crestal bone early likely matters more than chasing the perfect graft material. The graft families we use — xenograft (deproteinized bovine bone mineral), autograft chips from the surgical site, allograft, and synthetic alloplasts — are interchangeable for most cases.
Adjunctive technique worth knowing. A-PRF and L-PRF (platelet-rich fibrin, made from a small amount of your own blood spun in a centrifuge) are increasingly used alongside particulate grafts. Randomised trials suggest faster early healing and possibly higher early implant stability. They do not replace graft material in larger augmentations and have not shown a definitive long-term survival advantage, but they are a useful adjunct.
At our clinic. Lateral approach when RBH is below 5 mm. Transcrestal when 5–8 mm. CBCT-based planning on every case. We discuss bone augmentation before implant placement options openly with patients — graft material types, healing timelines, what the surgical recovery looks like — before any procedure is scheduled.
What recovery looks like — and the realistic risks
Recovery from a well-performed sinus lift is similar in feel to recovery from a wisdom tooth extraction. Most Swedish patients we treat describe day three or four as the worst day, with significant improvement by day seven. Travel home is usually comfortable by day two.
Typical timeline:
- · Day 0: procedure performed under local anaesthesia (with optional sedation). Patient returns to the hotel or home the same day.
- · Days 1–7: mild to moderate swelling, possible bruising over the cheek. Soft diet. Avoid nose-blowing — pressure can dislodge the graft. Antibiotic and anti-inflammatory regimen.
- · Weeks 2–4: sutures dissolve or are removed at the week 1–2 visit. Swelling resolves. Normal activity resumed.
- · Months 4–9: the graft integrates. CBCT at 6–9 months confirms readiness for implant placement, if it was not placed at the same session.
The realistic risk profile:
- · Membrane perforation — ~15–20% in lateral, ~3–5% in transcrestal, in experienced hands. Usually repaired intraoperatively with a collagen membrane. Rarely requires aborting the procedure.
- · Acute postoperative sinusitis — typically 1–3% incidence, with under 5% as the upper bound. Treated with antibiotics; usually resolves without complication.
- · Graft infection — roughly 2–5%, and higher in active smokers. This is the reason we recommend smoking cessation for 4–8 weeks before the procedure as best practice.
- · Graft non-integration — uncommon. Requires re-grafting.
Useful predictors of complications, worth flagging during CBCT planning:
- · Residual bone height under 3.5 mm
- · Presence of sinus septa
- · Sinus membrane thickness over 2 mm — elevated perforation risk
- · Membrane thickness over 5 mm — warrants ENT consultation before augmentation
Who should not have a sinus lift:
- · Patients with an active sinus infection (must be treated first)
- · Untreated periodontal disease
- · Heavy uncontrolled smoking (relative contraindication, strongly discouraged)
- · Certain autoimmune conditions affecting bone healing
Patient reassurance worth stating directly. Pjetursson et al. 2008 reported roughly 90% implant survival at 3 years; longer-term reviews report survival in the mid-90s%. This is statistically comparable to implants placed in non-augmented posterior maxilla when case selection, primary stability, and healing time are respected (Wallace & Froum 2003; Del Fabbro et al. 2004). A sinus lift does not produce inferior implants. It produces implants that work the same way as any other implant — they just needed a different starting point.
Honest framing per voice guide §5:
We will not pretend a sinus lift is a small thing. It is real surgery with real recovery. But it is also one of the most predictable bone augmentation procedures in modern implant dentistry, with success rates above 90% in the peer-reviewed literature. Most Swedish patients we treat do not regret having had it done.
A sinus lift performed by a non-specialist is one of the more common dental-tourism complication cases we see in second-opinion consultations. Done well, it is routine. Done badly, it can result in chronic sinusitis or graft failure that costs more to fix than the original implant treatment. If you are considering implant treatment in the upper back jaw, you can get a CBCT-based assessment from a named specialist with a verifiable BDIZ EDI / European Expert in Implantology credential. Prof. Robert Ćelić, European Expert in Implantology reviews cases personally in a free 30-minute consultation. No deposit, no commitment.
References
Sources referenced.
- Pjetursson BE, Tan WC, Zwahlen M, Lang NP (2008) — A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J Clin Periodontol 2008;35(8 Suppl):216–240. External link in H2.1.
- 1177.se — Konstgjorda tänder. Sweden's national health information service, patient-facing lay reference for artificial teeth and implants.
- Wallace SS, Froum SJ (2003) — Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol 2003;8(1):328–343. PMID 14971260. Average implant survival 91.8% (range 61.7–100%) with the lateral window technique; rough-surfaced implants outperform machined. Cited in the text.
- Del Fabbro M, Testori T, Francetti L, Weinstein R (2004) — Systematic review of survival rates for implants placed in the grafted maxillary sinus. Int J Periodontics Restorative Dent 2004;24(6):565–577. PMID 15626319. Overall implant survival 91.5%; up to ~96% with bone-substitute grafts and rough-surfaced implants; no single biomaterial consistently superior. Cited in the text.
- Short implants RCTs (multiple 2018–2024) — 6 mm implants as comparable alternative to sinus augmentation when RBH 6–8 mm. In-text only.
- Modern A-PRF / L-PRF systematic reviews — adjunctive use, faster early healing, no proven long-term survival advantage. In-text only.
Read next
Three pages worth your time.
The Pezo–Ćelić Protocol
Dental implants in Croatia — 20-year written guarantee
The full offer stack, dual guarantees, and surgeon-team accountability detailed.
Named credentials
Prof. Ćelić, European Expert in Implantology
Full Professor at University of Zagreb. BDIZ EDI certified. 916+ citations.
Related article
Osseointegration — how an implant fuses with the jawbone
What the bone actually does around the implant once the sinus lift has healed and the screw is placed.
Frequently asked questions
What is a sinus lift and why do some implant patients need one?
Do I always need a sinus lift for an upper back tooth implant?
What is the difference between a lateral window and a transcrestal sinus lift?
Is a sinus lift dangerous? What are the real risks?
How long is recovery after a sinus lift?
Do implants placed in a sinus lift site work as well as normal implants?
Ready when you are
Want a CBCT-based assessment from a named specialist?
A free 30-minute consultation. Send us your X-rays or current treatment plan. We will review it, give you our honest assessment, and confirm whether you are a candidate. If we do not think we are the right fit for your case, we will say so.
No deposit. No commitment.